
An article I co-wrote “More doctors should engage with arts in health” was recently published in BMJ careers. A longer version is below. Many healthcare professionals are interested in the arts, as part of their own wellbeing as well as their patients. It may not be clear how to align this interest with day to day work, and arts in health practice can therefore seem inaccessible to clinicians. We hope to bridge this gap with an introductory training event, the first of which will be on 30th June at the UCL Macmillan Cancer Centre, and has been approved for 3 RCP CPD points. Read more about it on the LAHF website, and book tickets via EventBrite.

What is good health?
Doctors spend their professional lives trying to help their patients achieve good health. Although many start medical school with an idealised image of medicine as cure, most rapidly realise that despite phenomenal advances in science, cure is seldom possible. This is partly due to the nature of disease and the inevitable frailty of the human body, and partly due to the fact that none of us exist in a vacuum, and our potions and pills do nothing to change individual patients’ contexts or experience of illness. In fact ‘illness’ is almost impossible to define, as we medicalise more and more natural life processes and events. How can medicine address modern day phenomena of socioeconomic inequalities, lack of housing, poverty, loneliness, ageing, grief, disengagement from society, struggles with sexuality, or finding meaning in life? Should it?
The role of the doctor has historically been to promote, maintain and restore health where possible, and to relieve suffering, and offer comfort to all. In this context, wellbeing as a concept that extends beyond a narrow definition of health becomes increasingly important. The WHO definition of health acknowledges this, and states that health is “a complete state of physical, mental and social wellbeing, and not merely the absence of disease or infirmity.”[1]
The Gallup Global Wellbeing index attempts to quantify aspects of wellbeing and compare across borders, languages and cultures. It defines five elements of well-being;
- purpose (liking what you do each day and being motivated to achieve your goals)
- social (having supportive relationships and love in your life)
- financial (managing your economic life to reduce stress and increase security)
- community (liking where you live, feeling safe and having pride in your community)
- physical (having good health and enough energy to get things done daily)
Medicine, as traditionally imagined, only addresses the last of these. Perhaps the social and creative potential of the arts could be harnessed to support the other elements and help physicians to generate a more holistic approach to health in our patients and communities.
What is arts in health practice?
Over recent years, there has been a growing understanding of the impact that taking part in the arts can have on health and wellbeing. By supplementing medicine and care, the arts can improve the health of people who experience mental or physical health problems. Engaging in the arts can promote prevention of disease and build wellbeing. The arts can improve healthcare environments and benefit staff retention and professional development. Arts in Health practice includes a wide range of approaches, projects, disciplines and professionals. It is much broader than what would traditionally be understood as medical humanities.

What is the evidence for the impact of arts and health initiatives?
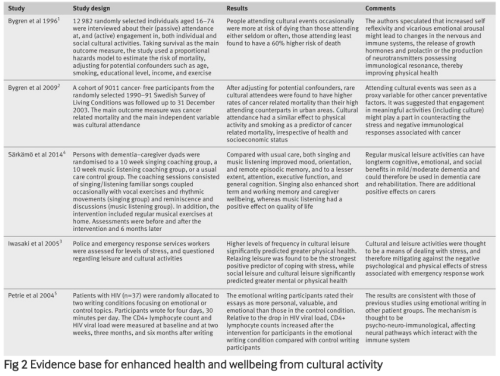
The arts have been recognised as central to wellbeing, but there is a lack of engagement from health professionals. Multiple contributing factors include: a lack of curricular time in undergraduate and postgraduate training for arts and health; a lack of interest, expertise, and leadership from clinically trained professionals and educators; poor funding; and institutional priorities. Although many successful arts in health projects exist, with years of experience and anecdotal evidence, those trained in positivist empirical scientific disciplines demand randomised controlled trials and objective evidence of impact before they invest time, energy, and crucially money, in initiatives that may be seen as ‘soft’. This stance, and the tendency to see arts engagement as ‘an intervention’ rather than a part of a long-term personal and therapeutic activity, leads to the prevailing narrative that a link between engagement in the arts and measurable physical and psychological outcomes is lacking. In fact such evidence already exists; there are numerous examples of the measurable impact of arts on health and wellbeing [6-9], in addition to specific effects of individual programmes which include RCTs [10-12]. (Table 1). A DoH working group in 2007 recognised this and stated “the arts are and should be firmly recognised as being integral to health, healthcare provision and healthcare environments.” [13]
Dr Gorden-Nesbitt of Manchester Metropolitan University reviewed the evidence for longitudinal effects of the arts on health and concluded “Taken together, the research demonstrates a positive association between engagement in high-quality arts activities and life expectancy, disease resistance, (and) mental acuity .” Possible mechanistic explanations include enhanced social capital, psycho-neuroimmunological responses, and epigenetic phenomena [6].

Why now?
Despite concerns about funding cuts to both healthcare and the arts, now is an exciting time for arts in health practice. There is increasing political interest in the area, with a recent All Party Parliamentary Group convened to explore Arts, Health and Wellbeing. The recent changes to the commissioning landscape are highly relevant. The Health and Social Care Act (2012) established Health and Wellbeing Boards with a remit of improving the health and wellbeing of their local populations. They have strategic influence over commissioning decisions across health, public health and social care, and offer potential for more cohesive, less silo-ed working. Importantly they have a remit to consider the social inequalities within their area, which remain huge determinants of health. Virchow famously stated “Medicine is a social science, and politics nothing but medicine at a larger scale.” [14] And as Dr Gordon-Nesbitt reflected “Whilst the arts and health inhabit two distinct policy areas, and the particularities of each field needs to be borne in mind, both health and the arts are inherently political. It follows that arts/health is a political movement…” [6]
How can you get involved in arts in health?
Having been won over to the inherent value of the arts, and the specific value of arts in health, how can you learn more and get involved? A number of options are open to you, dependant on your personal interests:
- Seek out information on local arts in health projects and take the opportunity to see them in action (the LAHF directory is a great place to start)
- Read more about Arts in Health, and the evidence base for enhanced health and wellbeing (see references below)
- Attend an event such as Medicine Unboxed, or Creativity and Wellbeing Week, to meet those involved in the field and find out more about the huge diversity of organisations and activities
- Contact your Trust’s arts manager/co-ordinator and find out what is happening locally
- Consider how you could incorporate the arts and enhance teaching you already have responsibility for, at an undergraduate or postgraduate level
- Advocate for including the arts in service reviews, whether this be participatory projects, physical environments, or arts therapies. Use examples of other projects, including The Kings Fund’s “Enhancing Healing Environments” to help your case.
For those with a particular interest in the field new ways to engage need to be developed. The London Arts in Health Forum are developing an introductory course for health practitioners who wish to learn more about the theory and practice of arts in health. The first of these will be on 30th June at the UCL Macmillan Cancer Centre and has been approved for 3 RCP CPD points. Read more about the event on the website and book tickets via EventBrite.
As Sir Peter Bazalgette, Chair of Arts Council England said, ‘When we talk about the value of arts and culture, we should always start with the intrinsic – how arts and culture illuminate our inner lives and enrich our emotional world. This is what we cherish. But while we do not cherish arts and culture because of the impact on our social wellbeing and cohesion, our physical and mental health […] they do confer these benefits and we need to show how important this is’. [6]
By facilitating front line health workers to become better equipped and engaged with arts in health, we can start to open opportunities for more individuals to reap the benefits of the arts, in all its forms. This has the potential to enhance life for us all: doctors, patients, public, and society at large.
- WHO. Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19-22 June 1946, and entered into force on 7 April 1948.
- Bircher J. Towards a dynamic definition of health and disease. Med. Health Care Philos 2005;8:335-41.
- Saracci R. The World Health Organization needs to reconsider its definition of Health. BMJ 1997;314:1409-10
- Department of Health. (1999). SavingLives: Our Healthier Nation. London: Stationery Office, (Cm 4386): 159pp.
- Smith R. Spend (slightly) less on health and more on the arts. BMJ. 2002 Dec 21;325(7378):1432–3.
- Gordon-Nesbitt R. Exploring the Longitudinal Relationship between Arts Engagement and Health. Available at: https://longitudinalhealthbenefits.wordpress.com/ accessed 20/09/15
- Arts Council England, The Value of Arts and Culture to People and Society: An Evidence Review (London: Arts Council England, 2014).
- Bygren, L. O., Konlaan, B. B., & Johansson, S. E. (1996). Attendance at cultural events, reading books or periodicals, and making music or singing in a choir as determinants for survival: Swedish interview survey of living conditions. BMJ: British Medical Journal, 313(7072), 1577.
- Bygren, L. O., Johansson, S-E., Konlaan, B.B., Grjibovski, A.M., Wilkinson, .V., & Sjöström, M.‘Attending Cultural Events and Cancer Mortality: A Swedish Cohort Study’, Arts & Health, 1, no. 1, March 2009, pp. 65–6.
- Iwasaki, Y., Mannell, R. C., Smale, B. J., & Butcher, J. (2005). Contributions of leisure participation in predicting stress coping and health among police and emergency response services workers. Journal of Health Psychology, 10(1), 79-99.
- Särkämö, T., Tervaniemi, M., Laitinen, S., Numminen, A., Kurki, M., Johnson, J. K., & Rantanen, P. (2014). Cognitive, emotional, and social benefits of regular musical activities in early dementia: Randomized controlled study. The Gerontologist, 54(4), 634-650.
- Petrie, K. J., Fontanilla, I., Thomas, M. G., Booth, R. J., & Pennebaker, J. W. (2004). Effect of written emotional expression on immune function in patients with human immunodeficiency virus infection: a randomized trial. Psychosomatic Medicine, 66(2), 272-275.
- Department of Health. Report of the review of arts and health working group. London: Department of Health, 2007.

