
Making and documenting good decisions about CPR (cardiopulmonary resuscitation) and treatment escalation plans, that are truly shared decisions, is a challenge. I find that the challenge comes from a number of factors: intrinsic difficulties of talking about the possibility of death in a largely death-denying culture; the great diversity of beliefs, wishes, and level of preparation for such decisions amongst patients; difficulties in facing my own mortality and the ways in which personal situations may affect my professional abilities; navigating tensions between hope and acceptance; and additional complexities that stem from having such conversations in the context of an emergency hospital admission. In the midst of a busy shift, faced with distressed people who are in pain, sometimes it is hard to find the words.
A number of recent cases have highlighted concerns about the process of resuscitation decision making and documentation. In particular, people have been distressed by the fact that DNACPR (do not attempt cardiopulmonary resuscitation) orders have being placed in their records without an explicit discussion with either them or their family. The High Court Ruling on R (David Tracey) vs 1) Cambridge University Hospitals 2) Secretary of State for Health forced the medical profession to face up to residual paternalism in this area of practice, and to make changes. It prompted some important reflections amongst individuals, teams and institutions and I have seen a noticeable difference in practice since the ruling, which reinforced the legal duty to discuss decisions about care with patients, particularly DNACPR decisions.
![]()
DNACPR discussions provide an opportunity to engage patients in informed decision making. This requires an awareness of what CPR is and what determines success. Unfortunately there is a wide gap between the practice and success rates of CPR on television, and reality [1,2]. Worse still, this gap has widened in recent years [3]. With this backdrop, it is essential that discussions between healthcare professionals and patients and their loved ones are open, honest, realistic, supportive and clear. A number of reports have questioned whether the processes and documents we use currently are adequate to support such discussions. For example The Health Select Committee’s enquiry into end-of-life care reported:
“We recommend that the Government review the use of DNACPR orders in acute care settings, including whether resuscitation decisions should be considered in the context of overall treatment plans. This Committee believes there is a case for standardising the recording mechanisms for the NHS in England.”
This has led to the development of a newly designed Emergency Care and Treatment Plan. The Resuscitation Council (UK) is currently holding a public consultation on this document and the information provided alongside it. Documents and guidelines have an authority and power that should not be underestimated; their language and structures shape our behaviour and frame our interactions. It is essential, therefore, that the panel considering new documentation on decisions regarding treatment during serious illness get it right. But what does ‘right’ look like? I have read the proposed document and it is has clearly been drawn up with good intentions. There are several aspects which would improve clarity and communication. However, the language used at the heart of the document leaves me concerned. I can see the benefits of widening the question beyond a yes/no decision on CPR, to encompass overall priorities for treatment. But, for me as a potential patient, and as a doctor in its’ current form the wording doesn’t capture the essence of these decisions in a way that will positively support clarity of communication.
Following discussions on CPR and other interventions, what I hope to capture in my documentation is the values of the patient, and any lines that they do not wish to cross. The current proposal requires a decision between three options:
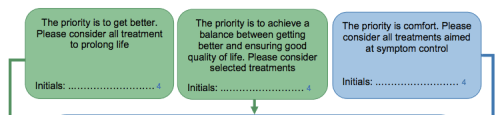
Although I could fit in any discussion to these categories I worry that they do not prompt and support relevant choice and accurately capturing the priorities of patients and their families. Most people’s priority is to get better, but this is not always possible or realistic. Who would not want to ‘consider’ all treatment to prolong life if framed in this way? I am concerned that the alternative options are too broad and therefore do not really help in this area of complex decision making. Although of course the document would be part of wider, more detailed discussions, these key headline categories could be a hindrance rather than a help in this process. I have suggested that the panel consider stronger wording and tentatively suggested:
- The over-riding priority is to prolong life, and all treatment options, no matter how invasive would therefore be accepted.
- The priority is to prolong life, but not at the cost of quality of life. Some interventions would not be accepted (see below for specifics).
- The over-riding priority is quality of life, therefore interventions which may prolong life but at the cost of quality of life would not be accepted. Care should be focused on symptom control, comfort and dignity.
These are in some ways subtle changes, but for me these statements are clearer and give a better sense of priorities, prompting documentation of more specific details. They also bring to the fore the real chance of harm from invasive interventions and ensure this forms part of decision making. I do not imagine everyone will agree, and I don’t think this formulation is perfect. I would be very interested to hear what others feel about the proposal.
The consultation closes at 9am on 29th February. Please consider submitting a response, particularly if you are a patient or carer. We need many voices and perspectives to make sure we find the right words and get this right.
- Harris, D., & Willoughby, H. (2009). Resuscitation on television: Realistic or ridiculous? A quantitative observational analysis of the portrayal of cardiopulmonary resuscitation in television medical drama. Resuscitation,80(11), 1275-1279.
- Hinkelbein, Jochen, et al. “An assessment of resuscitation quality in the television drama Emergency Room: Guideline non-compliance and low-quality cardiopulmonary resuscitation lead to a favorable outcome?.”Resuscitation 85.8 (2014): 1106-1110.
- Portanova, J., Irvine, K., Yi, J. Y., & Enguidanos, S. (2015). It isn’t like this on TV: Revisiting CPR survival rates depicted on popular TV shows.Resuscitation, 96, 148-150.


important topic, sadly my mother’s clear wishes in an AD and my presence as a health proxy still did not stop doctors use ‘best interest’ to over-riide good pain control…..still want to learn how to prevent this kind of thing happening again. if only the mental capacity act was properly implemented.who is working to achieve this?
I’m so sorry to hear that. It is fantastic that your mother had an advance directive, and it is clear that you knew her wishes. It is so sad to hear that, despite this, she suffered pain. I think there is greater awareness of the mental capacity act now but change is slow, and not uniform. I hope we can all work together to ensure people have choice, compassion and freedom from pain at the end of life.